


|
Having a history of benign (non-cancerous) breast disease can increase the chances of developing breast cancer. However, researchers have found that taking hormone replacement therapy (HRT) does not further increase the risk for breast cancer among post-menopausal women with proliferative breast disease. Proliferative breast disease (also called hyperplasia) is a non-cancerous condition characterized by an increase in the number of breast cells.
There is also an increased risk of breast cancer among women with benign breast disease, according to lead researcher Celia Byrne, PhD of Brigham and Women's Hospital and Harvard Medical School and her colleagues. To conduct the study, researchers analyzed biopsy cell samples from 133 post-menopausal breast cancer cases and 610 women with a history of benign breast disease. While they found that the risk of breast cancer was nearly double among women who had fast-growing proliferative breast disease versus women with slow-growing proliferative breast disease, the addition of HRT did not seem to further increase breast cancer risk. The breast cells of proliferative breast disease may be normal or abnormal. Proliferative breast disease with abnormal cells is called atypical hyperplasia. According to the researchers, the women with atypical hyperplasia were 3.6 times more likely to develop breast cancer than women with non-proliferative breast disease. 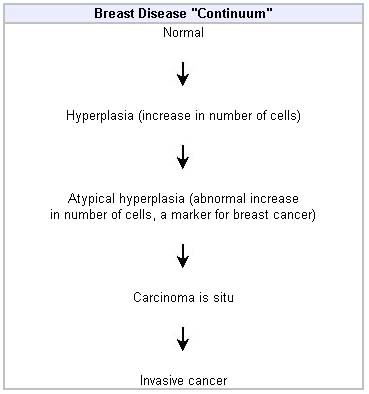 Many physicians think of breast disease as a continuum. Research has shown that many or most breast cancers do arise from the above sequence. However, some women with hyperplasia or atypical hyperplasia will never develop breast cancer. Also, some breast tumors may skip one or more intermediate steps (for example, they may proceed from normal directly to carcinoma in situ). In general, anything farther along than atypical hyperplasia is usually classified as a cancer. Abnormalities beginning with ductal carcinoma in situ (DCIS), usually require treatment as cancers. Benign breast disease is fairly common, though current or past use of HRT for five or more years did not further increase the risk of breast cancer among women with proliferative breast disease. However, researchers did not take into account different forms or doses of HRT. Many physicians recommend that women with atypical hyperplasia talk to their physicians about taking steps to help lower their breast cancer risk, especially if they have a strong family history of breast cancer or test positive for BRCA gene mutations. Preventive measures include frequent screenings, taking the drug tamoxifen, or considering a prophylactic mastectomy (preventive breast removal). However, having fibrocystic breasts, a benign breast condition that affects nearly 50% of women at some point in their lives, is not a risk factor for breast cancer. Guidelines for early breast cancer detection:
|
