


Patients with coronary artery disease (CAD) often show no symptoms before experiencing myocardial infarction (heart attack). Approximately 50% of men and 63% of women who die suddenly from CAD show no previous symptoms of the disease. The degree to which patients experience symptoms of CAD varies, if they experience any symptoms at all. Also, women tend to experience different symptoms than men.
Typically, patients are screened for CAD during routine office visits, even if the patient has no symptoms of heart disease. Detection may also take place in the emergency room if a patient experiences myocardial infarction (heart attack). In some cases, angina (chest pain) and dyspnea (shortness of breast) may accompany CAD. Other symptoms may include:
- tightness, heaviness, burning sensation, pressure, squeezing, or pain behind the breastbone or less commonly also in the arms, neck or jaws
- nausea and vomiting
- fatigue
- sweating
- weakness
CAD detection begins with a thorough physical exam, including careful documentation of family and personal history of heart problems and lifestyle factors, including smoking. In addition to a physical exam, blood cholesterol tests and blood pressure measurements are routinely used to help screen for CAD. Electrocardiogram and/or stress test may also be given. Recently, the U.S. government recommended aggressive new guidelines to help prevent heart disease. Click here to learn about the new guidelines.
Men have a greater risk of heart attack than women and are more likely to have heart attacks earlier in life
than women. However, women are also at risk for heart disease. As a woman ages, her risk of heart disease
increases: 9,000 American women under age 45 have heart attacks each year versus 250,000 women over age 65. Medical
experts believe the increased risk of heart disease in older women is related to the depletion of the female
hormone estrogen at menopause.
Many of the risk factors for heart disease are the same for women and men (see above section). However, other risk factors for women include menopause (specifically, loss of estrogen at this time) and the use of oral contraceptives among smokers or those with high blood pressure.
Women also tend to have different heart attack symptoms than men. The following chart summarizes these differences:
|
Heart Attack Symptoms | |
| In Both Men and Women | More Often in Women Only |
|
|
- Blood cholesterol: Blood tests to monitor cholesterol levels are typically performed once every five years for adults between the ages of 20 and 35 if the levels are normal. After age 35, cholesterol tests are typically monitored every two years or every year depending on age, family history, test results, etc.
| Total cholesterol (mg/dL) | LDL cholesterol (mg/dL) | HDL cholesterol (mg/dL) |
| Ideal: Less than 200
Borderline high risk: 200-239 High risk: 240 and over |
Ideal: less than 130
Borderline high risk: 130-159 High risk: 160 or higher |
Ideal: 60 or higher High risk: lower than 40 |
- Blood pressure: Blood pressure is usually taken during each office visit or other regular interval.
| (mm Hg) | Ideal | Normal | High Normal | Hypertension |
| Systolic (top number) | Less than 120 | Less than 130 | 130-139 | 140 or higher |
| Diastolic (bottom number) |
Less than 80 | Less than 85 | 85-89 | 90 or higher |
*source: American Heart Association
- Chest x-ray: A chest x-ray images the heart and surrounding thoracic anatomy, shows heart size and shape, and reveals whether the heart is misshaped or enlarged due to disease. Abnormal calcification (hardened blockage due to cholesterol build up) in the main blood vessels and fluid in the lungs (possible indication of congestive heart failure) can also be seen. Chest x-rays can also be used to image pacemakers and artificial heart valves to check for correct positioning.
- Electrocardiogram (ECG or EKG): An electrocardiogram is a graphical record of the electrical activity of the heart. A normal ECG, in most cases, rules out the presence of other cardiac diseases. An abnormal ECG indicates the presence of a cardiac disease and further investigations are performed. An ECG can be beneficial in detecting the disease and sometimes even the extent of the disease.
- Stress test: A stress test involves taking an EKG before, during and after a treadmill workout to detect possible cardiac disease and/or damage, including the extent of CAD. However, false positive results are possible with stress tests. A stress test is typically performed on adults 40 years of age or older who are at high risk for CAD.
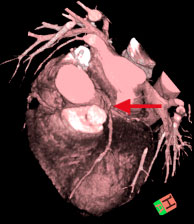 |
| This multi-slice CT image shows narrowing of the arteries (stonosis). Image courtesy of http://www.heartinformation.com |
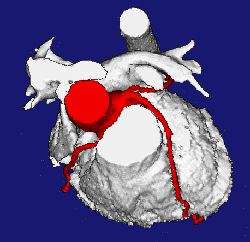 |
| 3D reconstructed heart showing coronary arteries in red, acquired with EBCT |
EBCT is a special type of computed tomography (CT) that uses a sweeping electron beam to create the rotating x-ray effect needed to make a computed tomography image. This makes EBCT different from conventional CT which has an x-ray tube mounted on a rotating frame. By using a sweeping electron beam, EBCT images can be acquired in as fast as 50 or 100 milliseconds, or some 10 times faster than the fastest slip-ring CT systems that can acquire an image in about 500 milliseconds. In order to image the beating heart and eliminate all image degradation caused by heart motion, image acquisition time must be in the 100 millisecond or faster range. In other words, a conventional slip-ring CT scanner can acquire one to two image per second while an EBCT system can acquire at a much faster rate of 10 to 20 images per second.
- Ambulatory monitoring: If no abnormality, disease or damage is detected and the patient still feels uneasy when performing stressful activities (such as climbing stairs) but feels okay under normal activity, then an ambulatory monitor may be used. An ambulatory monitor is a portable EKG system (often worn around the waist) that continuously monitors the heart’s electrical activity.
Updated: Updated: February 29, 2008
